
Bladder Cancer
About Bladder Cancer
Key Points
- Bladder cancer is a disease in which malignant (cancer) cells form in the tissues of the bladder.
- Smoking can affect the risk of bladder cancer.
- Signs and symptoms of bladder cancer include blood in the urine and pain during urination.
- Tests that examine the urine and bladder are used to help detect (find) and diagnose bladder cancer.
- Certain factors affect prognosis (chance of recovery) and treatment options.
Bladder cancer is a disease in which malignant (cancer) cells form in the tissues of the bladder.
The bladder is a hollow organ in the lower part of the abdomen. It is shaped like a small balloon and has a muscular wall that allows it to get larger or smaller to store urine made by the kidneys. There are two kidneys, one on each side of the backbone, above the waist. Tiny tubules in the kidneys filter and clean the blood. They take out waste products and make urine. The urine passes from each kidney through a long tube called a ureter into the bladder. The bladder holds the urine until it passes through the urethra and leaves the body.
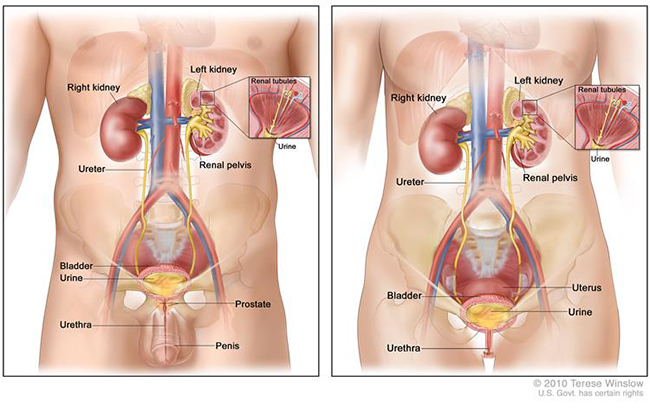
Anatomy of the male urinary system (left panel) and female urinary system (right panel) showing the kidneys, ureters, bladder, and urethra. Urine is made in the renal tubules and collects in the renal pelvis of each kidney. The urine flows from the kidneys through the ureters to the bladder. The urine is stored in the bladder until it leaves the body through the urethra.
There are three types of bladder cancer that begin in cells in the lining of the bladder. These cancers are named for the type of cells that become malignant (cancerous):
- Transitional cell carcinoma: Cancer that begins in cells in the innermost tissue layer of the bladder. These cells are able to stretch when the bladder is full and shrink when it is emptied. Most bladder cancers begin in the transitional cells. Transitional cell carcinoma can be low-grade or high-grade:
- Low-grade transitional cell carcinoma often recurs (comes back) after treatment, but rarely spreads into the muscle layer of the bladder or to other parts of the body.
- High-grade transitional cell carcinoma often recurs (comes back) after treatment and often spreads into the muscle layer of the bladder, to other parts of the body, and to lymph nodes. Almost all deaths from bladder cancer are due to high-grade disease.
- Squamous cell carcinoma: Cancer that begins in squamous cells, which are thin, flat cells that may form in the bladder after long-term infection or irritation.
- Adenocarcinoma: Cancer that begins in glandular (secretory) cells that are found in the lining of the bladder. This is a very rare type of bladder cancer.
Cancer that is in the lining of the bladder is called superficial bladder cancer. Cancer that has spread through the lining of the bladder and invades the muscle wall of the bladder or has spread to nearby organs and lymph nodes is called invasive bladder cancer.
See the following PDQ summaries for more information:
- Renal cell cancer treatment
- Transitional cell cancer of the renal pelvis and ureter treatment
- Bladder and other urothelial cancers screening
- Unusual cancers of childhood treatment
Signs and symptoms of bladder cancer include blood in the urine and pain during urination.
These and other signs and symptoms may be caused by bladder cancer or by other conditions. Check with your doctor if you have any of the following:
- Blood in the urine (slightly rusty to bright red in colour).
- Frequent urination.
- Pain during urination.
- Lower back pain.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis (chance of recovery) depends on the following:
- The stage of the cancer (whether it is superficial or invasive bladder cancer, and whether it has spread to other places in the body). Bladder cancer in the early stages can often be cured.
- The type of bladder cancer cells and how they look under a microscope.
- Whether there is carcinoma in situ in other parts of the bladder.
- The patient’s age and general health.
If the cancer is superficial, prognosis also depends on the following:
- How many tumours there are.
- The size of the tumours.
- Whether the tumour has recurred (come back) after treatment.
Treatment options depend on the stage of bladder cancer.
Smoking can affect the risk of bladder cancer.
Anything that increases your chance of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn’t mean that you will not get cancer. Talk to your doctor if you think you may be at risk for bladder cancer.
Other risk factors for bladder cancer include:
- Using tobacco, especially smoking cigarettes.
- Having a family history of bladder cancer.
- Having certain changes in the genes that are linked to bladder cancer.
- Being exposed to paints, dyes, metals, or petroleum products in the workplace.
- Past treatment with radiation therapy to the pelvis or with certain anticancer drugs, such as cyclophosphamide or ifosfamide.
- Taking Aristolochia Fangchi, a Chinese herb.
- Drinking water from a well that has high levels of arsenic.
- Drinking water that has been treated with chlorine.
- Having a history of bladder infections, including bladder infections caused by Schistosoma haematobium.
- Using urinary catheters for a long time.
Older age is a risk factor for most cancers. The chance of getting cancer increases as you get older.
Stages of Bladder Cancer
Key Points
After bladder cancer has been diagnosed, tests are done to find out if cancer cells have spread within the bladder or to other parts of the body.
There are three ways that cancer spreads in the body.
Cancer may spread from where it began to other parts of the body.
The following stages are used for bladder cancer:
- Stage 0 (Papillary Carcinoma and Carcinoma in Situ)
- Stage I
- Stage II
- Stage III
- Stage IV
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumour) and travel through the lymph system or blood.
- Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumour (metastatic tumour) in another part of the body.
- Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumour (metastatic tumour) in another part of the body.
The metastatic tumour is the same type of cancer as the primary tumour. For example, if bladder cancer spreads to the bone, the cancer cells in the bone are actually bladder cancer cells. The disease is metastatic bladder cancer, not bone cancer.
The following stages are used for bladder cancer:
Stage 0 (Papillary carcinoma and carcinoma in situ)
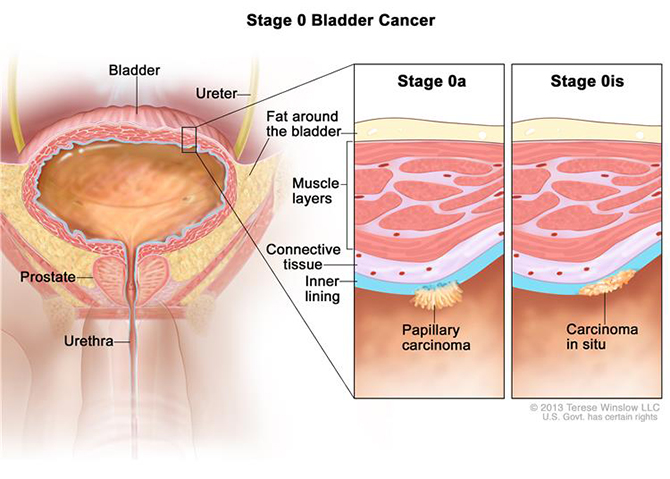
Stage 0 bladder cancer. Abnormal cells are found in the tissue lining the inside of the bladder. Stage 0a may look like tiny mushrooms growing from the lining of the bladder. Stage 0is is a flat tumour on the tissue lining the inside of the bladder.
In stage 0, abnormal cells are found in tissue lining the inside of the bladder. These abnormal cells may become cancer and spread into nearby normal tissue. Stage 0 is divided into stage 0a and stage 0is, depending on the type of the tumour:
- Stage 0a is also called papillary carcinoma, which may look like tiny mushrooms growing from the lining of the bladder.
- Stage 0is is also called carcinoma in situ, which is a flat tumour on the tissue lining the inside of the bladder.
Stage I
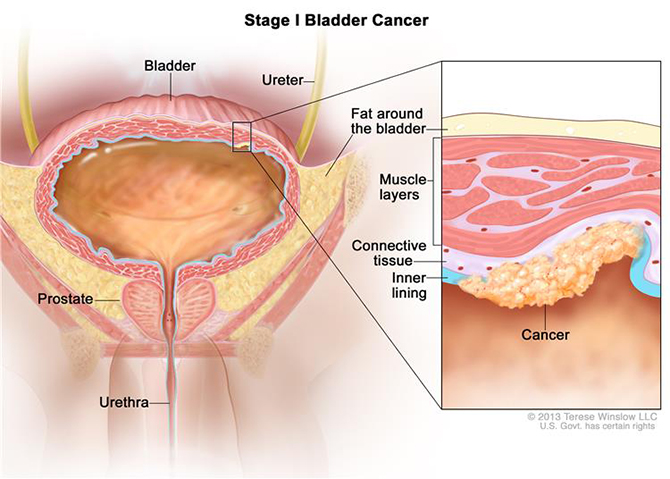
Stage I bladder cancer. Cancer has spread to the layer of connective tissue next to the inner lining of the bladder.
In stage I, cancer has formed and spread to the layer of connective tissue next to the inner lining of the bladder.
Stage II
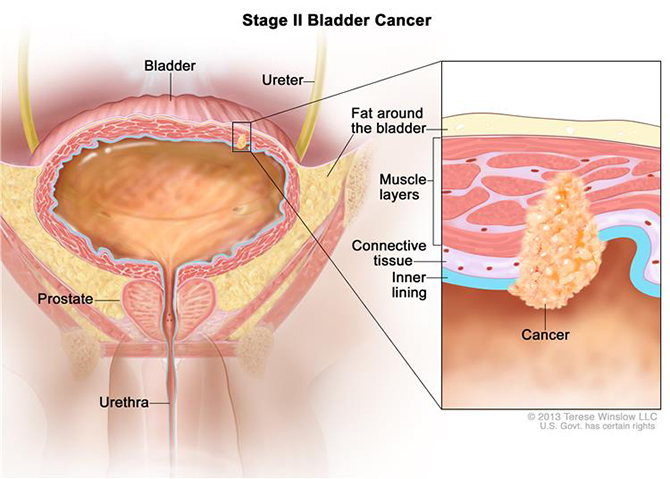
Stage II bladder cancer. Cancer has spread to the layers of muscle tissue of the bladder.
In stage II, cancer has spread to the layers of muscle tissue of the bladder.
Stage III
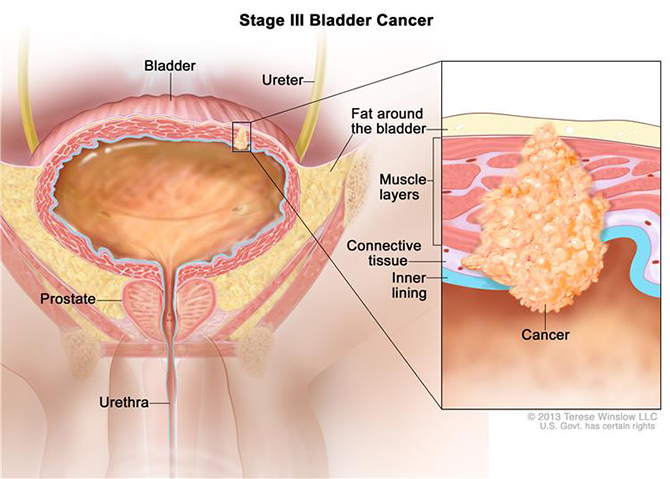
Stage III bladder cancer. Cancer has spread from the bladder to the layer of fat surrounding it. It may also have spread to the prostate and/or seminal vesicles in men or the uterus and/or vagina in women.
In stage III, cancer has spread from the bladder to the layer of fat surrounding it and may have spread to the reproductive organs (prostate, seminal vesicles, uterus, or vagina).
Stage IV
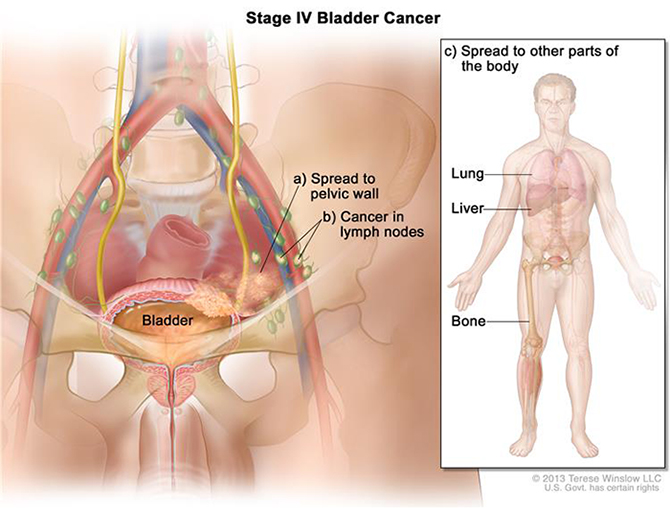
Stage IV bladder cancer. Cancer has spread from the bladder to (a) the wall of the abdomen or pelvis, (b) one or more lymph nodes, and/or (c) other parts of the body, such as the lung, liver, or bone.
In stage IV, one or more of the following is true:
- Cancer has spread from the bladder to the wall of the abdomen or pelvis.
- Cancer has spread to one or more lymph nodes.
- Cancer has spread to other parts of the body, such as the lung, bone, or liver.
Recurrent Bladder Cancer
Recurrent bladder cancer is cancer that has recurred (come back) after it has been treated. The cancer may come back in the bladder or in other parts of the body.
Bladder Cancer Diagnosis & Screening
Biopsy
Biopsy of the bladder is usually done during cystoscopy. It may be possible to remove the entire tumour during biopsy.
Bone Scan
Your doctor may want to see if the cancer has metastasised and has affected your bones. A small amount of radioactive material is injected into your arm; Abnormal bone absorbs more of the radioactive substance than normal bone and shows up on the scan as highlighted areas (known as ‘hot spots’). Your arm will then be scanned an hour later to view the activity of the bone and ascertain whether the cancer has spread.
The level of radioactivity that is used is very small and does not cause any harm.
This scan can also detect other conditions affecting the bones such as arthritis, so further tests such as an x-ray of the abnormal area may be necessary to confirm that it is cancer.
CT Scan
CT scan is basically an x-ray tube that rotates in a circle around the patient and takes a series of pictures as it rotates. The multiple x-ray pictures are reconstructed by a computer in axial slice images at different levels. Each level can be examined separately.
A CT scan may show if the cancer has spread beyond the prostate to other parts of the body such as the lymph nodes.
The scan takes from 10-30 minutes. You may be given a drink or injection of a dye, which allows particular areas to be seen more clearly. For a few minutes, this may make you feel hot all over. If you are allergic to iodine or have asthma you could have a more serious reaction to the injection, so it is important to let your doctor know beforehand.
You will probably be able to go home as soon as the scan is over.
Pathology/Urinalysis
Following your first or subsequent visit to Prof Patel you may be asked for a blood or urine test. Below are a few common tests that may be prescribed.
Blood tests
Some of the more common blood tests are:
FBC (Full Blood Count): The haemoglobin level is checked and the different blood cells are looked at in detail under the microscope. Various forms of anaemia are picked up as are viral infections like glandular fever. People on some medications require regular FBE’s.
UEC’s (Urea Electrolytes and Creatinine): This test is a measure of kidney function. We see an elevated serum urea or creatinine with dehydration or if the kidney functions are impaired. The electrolytes are the various salts in the bloodstream, things like sodium, potassium, chloride and bicarbonate. The potassium level is of particular importance in people on diuretics or fluid tablets. Frequently the level falls in these patients and oral potassium supplements are required.
Blood tests to check the levels of certain hormones might be prescribed to determine the cause of
- Impotence
- Recurrent urinary stones
- Uro-gynaecological cases
Urinalysis
A urinalysis is an analysis of the urine. A series of physical, microscopic, and chemical tests are conducted on a sample of urine. The tests can screen for kidney disease and infections of the urinary tract. They can also help diagnose diseases that produce abnormal breakdown products called metabolites that are passed from the body into the urine.
Urine culture
Urine culture help identify organisms that cause infection that may be present in urine.
The culture may be ordered when:
- Symptoms indicate the possibility of a urinary tract infection, such as pain and burning when urinating and frequent urge to urinate
- Patients have a catheter inserted for an extended period of time, even if they do not show overt symptoms of an infection, since there is a risk of bacteria being introduced via the catheter
- Pregnant women without any symptoms may be screened for bacteria in their urine, which could harm the baby
If you have urinary tract infection (UTI), antibiotic susceptibility testing is usually done to determine the resistance of bacteria (germs).
A clean catch or mid-stream sample of urine should be used for urinalysis.
Bladder Cancer Treatments
Surgery
There are a number of treatments available to patients diagnosed with bladder cancer. Treatment depends on whether the bladder cancer is early and limited to the initial layers of the bladder or whether it has invaded into the deeper muscle layer of the bladder. The choice of treatments depends on a number of factors, including age, general health and the extent and stage of the tumour. Prof Patel will ascertain the most appropriate course of treatment for you.
Cystoscopy
Cystoscopy enables Prof Patel to directly view the inside of the urinary bladder and urethra in great detail using a “cystoscope” (the instrument used).
There are two types of cystoscope
- Rigid cystoscope: This is a solid straight telescope, which has been in use for many years. It is used alone with a high intensity light source and a separate channel to allow other instruments to be attached
- Flexible cystoscope: This is more commonly used particularly for diagnosis and for the follow up of most bladder tumours. It is a fibre optic instrument that can bend easily and has a manoeuvrable tip that makes it easy to pass along the curves of the urethra
This procedure may be carried out under general anaesthetic. The use of flexible instruments may allow, in some cases, the procedure to be carried out under local anaesthetic on an outpatient basis. Cystoscopy may be indicated for the following conditions
- Frequent urinary tract infections
- Blood in your urine (haematuria)
- Loss of bladder control (incontinence) or overactive bladder
- Unusual cells found in urine sample
- Need for a bladder catheter
- Painful urination, chronic pelvic pain, or interstitial cystitis
- Urinary blockage such as prostate enlargement, stricture, or narrowing of the urinary tract
- Stone in the urinary tract
- Unusual growth, polyp, tumour, or cancer
TURBT
If a tumour in the bladder is diagnosed on imaging or at cystoscopy, a sample of the growth is required. If it is small, only a small biopsy is required followed by cauthery to stop it bleeding.
If it is larger however it will need to be resected. This is performed by inserting a telescope through the urethra and cutting the tumour into little pieces prior to removing it from the bladder and sending it for pathological evaluation. The results will allow Prof Patel to determine the next course of treatment required.
After the TURBT, it is common to require a catheter for 1-2 days After it is removed and you are sent home, there can be blood in the urine (for up to two weeks after the procedure), and some pain/burning on urination.
Radical Cystectomy
When the bladder cancer has grown or invaded surrounding muscle or tissue surgical management is most likely to be necessary, usually in the form of a cystectomy which is the complete removal of the bladder.
Radical cystectomy involves removal of the entire bladder and in women also the uterus, fallopian tubes, ovaries, anterior vaginal wall (the front of the birth canal), and urethra.
In men, if the prostate and bladder are both removed the procedure is known as cysto-prostatectomy.
With a radical cystectomy, removing the bladder and surrounding organs will change the way the body functions. In men, the nerves needed to get an erection are likely to be affected. Women who have their reproductive organs removed will go through menopause if they have not already.
Robotic radical cystectomy is a new advanced laparoscopic (key hole) approach that enables the surgeon to perform complex surgery through tiny incisions, with precision and ease, improving the outcome and reducing complications.
About the robot
Robotic surgery involves two machines, a control unit or the surgeon’s console and a patient unit. The surgeon sits at the control unit, away from the operating table, and controls the movement of the four robotic arms of the patient unit, present near the operating table. One of the robotic armsholds and positions a 3D high definition camera through the incision in the operated area providing images of the operation site to the surgeon at the control unit. These images are high resolution 3D images, superior to the 2D images in the laparoscopic approach. Moreover, the images can also be magnified by 10 to 12 times. The other three robotic arms are used to hold small miniature instruments, which are used for the surgery. These instruments are introduced through the tiny (7mm) incisions over the patient’s abdomen. These miniature instruments are more flexible compared to the long handled rigid instruments of the traditional laparoscopic surgery. A wide range of these instruments are available to the surgeon to perform various specialised surgical tasks.
The robotic arm cannot be programmed to do the surgery on its own. Instead, it translates the surgeon’s hand movements, at the control unit, into precise movements of the micro-instruments in the operation site, minimising tremors that may occur from unintended shaking of the surgeon’s hands. The enhanced vision and superior control of the micro-instruments helps in precise removal of the cancer while limiting damage to the nerve fibres and the blood vessels near it.
What is Urinary Diversion?
A urinary diversion is necessary when the bladder is removed to divert the flow of urine.
Types of Urinary Diversions
Once the bladder is separated from the ureters and urethra, it is necessary to provide another way to collect and drain the urine. Several options exist and depend on the overall health of the patient, the extent of cancer, and an individual’s motivation and active participation in their care.
In selected patients, a portion of the intestines is used to create a new bladder or neo-bladder. The ureters are joined to one end of the neo-bladder and the other end is connected to the remaining portion of the urethra. The new bladder is constructed in such a way that it will provide a reservoir to store urine and control urine flow. You may urinate in much the same way you do now.
For patients who receive the neo-bladder, you will notice that you will not be able to hold any urine in the neo-bladder initially. This is temporary. Please buy incontinence pads or pull-ups for the first few weeks to months after the surgery. Most patients will gain control of their urine within a few months.

Neobladder: Connection of new bladder to existing urethra. (image adapted from Campbell-Walsh Urology)

Ileal Conduit: Short segment of small intestine connecting ureters to skin. (image adapted from Campbell-Walsh Urology)

Ileal Conduit: Short segment of small intestine connecting ureters to skin. (image adapted from Campbell-Walsh Urology)
Some patients are better served by creating a simpler ileal conduit. This is created using a shorter portion of intestine between the ureters to a stoma connected to the side of the abdomen. It acts as a funnel to drain urine from the kidneys to an appliance bag attached to the patient’s skin. It has the disadvantages of requiring an ostomy bag, but is a shorter and simpler operation with the least chance of post-operative or long-term complications.
Intra-vesical Therapy
Intra-vesical treatment involves flushing the bladder with chemotherapy or immunotherapy to kill any residual tumour cells. In this procedure chemotherapy drugs are placed directly into the bladder in order to prevent the tumour recurring or to prevent it from invading the deeper layers of the bladder wall.
Intravesical chemotherapy is used only for non-muscle-invasive bladder cancer, as the chemotherapy delivered to the bladder cannot reach cancer cells in any surrounding tissues or cells that have spread to other parts of the body.
Chemotherapy
Chemotherapy concerns the use of special cytotoxic drugs to treat cancers by either killing the cancer cells or slowing their growth. Chemotherapy drugs travel round the body and attack rapidly growing cells, which may also include healthy cells in the body as well as cancer cells. However the breaks between bouts of chemo allow the bodies normal cells to recover before the next course of chemo.
To travel the body, chemotherapy needs to enter the bloodstream and the quickest way to do this is intravenously – through a vein or artery. Other methods of administering chemotherapy may also take the form of intra-muscular injections, tablets or creams. The way you have chemotherapy depends on a number of factors including the type of cancer you have and the drugs that you are taking. Talk with your doctor if you have any questions about your treatment regime.
Some cancers can be treated or cured by chemotherapy alone, while some treatments may combine chemotherapy with other procedures such as surgery or radiotherapy – this is known as adjuvant therapy. Adjuvant chemotherapy can be used before the main treatment to help make the tumour smaller, or after treatment to kill residual cancer cells that may cause problems later in treatment.
In some instances chemotherapy may not be able to control the cancer but may be used to relieve symptoms such as pain and help you lead as normal a life as is possible.
There are many different combinations of chemotherapy used to treat various cancers, and these may have different effects on different people.
Side effects of chemotherapy
While chemotherapy is useful for the killing of cancer cells in the body, as with most other treatments patients may experience side effects from the chemotherapy.
These side effects vary from treatment to treatment and from person to person but fortunately these problems may disappear with time or be managed to reduce the impact that they may cause.
The most common side effects are nausea and vomiting, fatigue (tiredness), alopecia (hair loss), muscular, nerve and blood effects as well as bowel (constipation or diarrhoea) and oral problems.
It is important that you tell the doctors and nurses if you are experiencing any side effects from your treatment so that they can discuss an appropriate course of action with you.
Radiotherapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy. External radiation therapy uses a machine outside the body to send radiation toward the cancer. Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer. The way the radiation therapy is given depends on the type and stage of the cancer being treated.
Treatment Options by Stage
Stage 0 (Papillary Carcinoma and Carcinoma in Situ)
Treatment of stage 0 (papillary carcinoma and carcinoma in situ) may include the following:
- Transurethral resection with fulguration. This may be followed by one of the following:
- Intravesical chemotherapy given right after surgery.
- Intravesical chemotherapy given right after surgery and then regular treatments with intravesical BCG or intravesical chemotherapy.
- Partial cystectomy.
- Radical cystectomy.
- A clinical trial of a new treatment.
Stage I Bladder Cancer
Treatment of stage I bladder cancer may include the following:
- Transurethral resection with fulguration. This may be followed by one of the following:
- Intravesical chemotherapy given right after surgery.
- Intravesical chemotherapy given right after surgery and then regular treatments with intravesical BCG or intravesical chemotherapy.
- Partial cystectomy.
- Radical cystectomy.
- A clinical trial of a new treatment.
Stages II and III Bladder Cancer
Treatment of stages II and III bladder cancer may include the following:
- Radical cystectomy.
- Combination chemotherapy followed by radical cystectomy. A urinary diversion may be done.
- External radiation therapy with or without chemotherapy.
- Partial cystectomy with or without chemotherapy.
- Transurethral resection with fulguration.
- A clinical trial of a new treatment.
Stage IV Bladder Cancer
Treatment of stage IV bladder cancer that has not spread to other parts of the body may include the following:
- Chemotherapy.
- Radical cystectomy alone or followed by chemotherapy.
- External-beam radiation therapy with or without chemotherapy.
- Urinary diversion or cystectomy as palliative therapy to relieve symptoms and improve quality of life.
Treatment of stage IV bladder cancer that has spread to other parts of the body, such as the lung, bone, or liver, may include the following:
- Chemotherapy with or without local treatment (surgery or radiation therapy).
- External-beam radiation therapy as palliative therapy to relieve symptoms and improve quality of life.
- Urinary diversion or cystectomy as palliative therapy to relieve symptoms and improve quality of life.
- A clinical trial of new anticancer drugs.
Treatment Options for Recurrent Bladder Cancer
Treatment of recurrent bladder cancer depends on previous treatment and where the cancer has recurred. Treatment for recurrent bladder cancer may include the following:
- Combination chemotherapy.
- Surgery for superficial or localised tumours. Surgery may be followed by biologic therapy and/or chemotherapy.
- Radiation therapy as palliative therapy to relieve symptoms and improve quality of life.
- A clinical trial of a new treatment.