
Penile Cancer
About Penile Cancer
Key Points
- Penile cancer is a disease in which malignant (cancer) cells form in the tissues of the penis.
- Human papillomavirus infection may increase the risk of developing penile cancer.
- Signs of penile cancer include sores, discharge, and bleeding.
- Tests that examine the penis are used to detect (find) and diagnose penile cancer.
- Certain factors affect prognosis (chance of recovery) and treatment options.
Penile cancer is a disease in which malignant (cancer) cells form in the tissues of the penis.
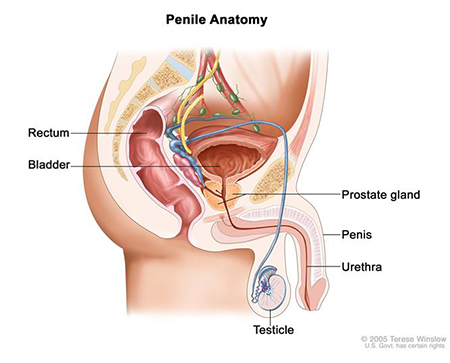
The penis is a rod-shaped male reproductive organ that passes sperm and urine from the body. It contains two types of erectile tissue (spongy tissue with blood vessels that fill with blood to make an erection):
- Corpora cavernosa: The two columns of erectile tissue that form most of the penis.
- Corpus spongiosum: The single column of erectile tissue that forms a small portion of the penis. The corpus spongiosum surrounds the urethra (the tube through which urine and sperm pass from the body).
The erectile tissue is wrapped in connective tissue and covered with skin. The glans (head of the penis) is covered with loose skin called the foreskin.
Signs of penile cancer include sores, discharge, and bleeding.
These and other signs may be caused by penile cancer or by other conditions. Check with your doctor if you have any of the following:
- Redness, irritation, or a sore on the penis.
- A lump on the penis.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis (chance of recovery) and treatment options depend on the following:
- The stage of the cancer.
- The location and size of the tumour.
- Whether the cancer has just been diagnosed or has recurred (come back).
Human papillomavirus infection may increase the risk of developing penile cancer.
Anything that increases your chance of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn’t mean that you will not get cancer. Talk with your doctor if you think you may be at risk. Risk factors for penile cancer include the following:
Circumcision may help prevent infection with the human papillomavirus (HPV). A circumcision is an operation in which the doctor removes part or all of the foreskin from the penis. Many boys are circumcised shortly after birth. Men who were not circumcised at birth may have a higher risk of developing penile cancer.
Other risk factors for penile cancer include the following:
- Being age 60 or older.
- Having phimosis (a condition in which the foreskin of the penis cannot be pulled back over the glans).
- Having poor personal hygiene.
- Having many sexual partners.
- Using tobacco products.
Stages of Penile Cancer
Key Points
- After penile cancer has been diagnosed, tests are done to find out if cancer cells have spread within the penis or to other parts of the body.
- There are three ways that cancer spreads in the body.
- Cancer may spread from where it began to other parts of the body.
- The following stages are used for penile cancer:
- Stage 0 (Carcinoma in Situ)
- Stage I
- Stage II
- Stage III
- Stage IV
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumour) and travel through the lymph system or blood.
- Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumour (metastatic tumour) in another part of the body.
- Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumour (metastatic tumour) in another part of the body.
The metastatic tumour is the same type of cancer as the primary tumour. For example, if penile cancer spreads to the lung, the cancer cells in the lung are actually penile cancer cells. The disease is metastatic penile cancer, not lung cancer.
The following stages are used for penile cancer:
Stage 0 (Carcinoma in Situ)
In stage 0, abnormal cells or growths that look like warts are found on the surface of the skin of the penis. These abnormal cells or growths may become cancer and spread into nearby normal tissue. Stage 0 is also called carcinoma in situ.
Stage I
In stage I, cancer has formed and spread to connective tissue just under the skin of the penis. Cancer has not spread to lymph vessels or blood vessels. The tumour cells look a lot like normal cells under a microscope.
Stage II
In stage II, cancer has spread:
- to connective tissue just under the skin of the penis. Also, cancer has spread to lymph vessels or blood vessels or the tumour cells may look very different from normal cells under a microscope; or
- through connective tissue to erectile tissue (spongy tissue that fills with blood to make an erection); or
- beyond erectile tissue to the urethra.
Stage III
Stage III is divided into stage IIIa and stage IIIb.
In stage IIIa, cancer has spread to one lymph node in the groin. Cancer has also spread:
- to connective tissue just under the skin of the penis. Also, cancer may have spread to lymph vessels or blood vessels or the tumour cells may look very different from normal cells under a microscope; or
- through connective tissue to erectile tissue (spongy tissue that fills with blood to make an erection); or
- beyond erectile tissue to the urethra.
In stage IIIb, cancer has spread to more than one lymph node on one side of the groin or to lymph nodes on both sides of the groin. Cancer has also spread:
- to connective tissue just under the skin of the penis. Also, cancer may have spread to lymph vessels or blood vessels or the tumour cells may look very different from normal cells under a microscope; or
- through connective tissue to erectile tissue (spongy tissue that fills with blood to make an erection); or
- beyond erectile tissue to the urethra.
Stage IV
In stage IV, cancer has spread:
- to tissues near the penis such as the prostate, and may have spread to lymph nodes in the groin or pelvis; or
- to one or more lymph nodes in the pelvis, or cancer has spread from the lymph nodes to the tissues around the lymph nodes; or
- to distant parts of the body.
Recurrent Penile Cancer
Recurrent penile cancer is cancer that has recurred (come back) after it has been treated. The cancer may come back in the penis or in other parts of the body.
Penile Cancer Diagnosis and Screening
The following tests and procedures may be used:
- Physical exam and history: An exam of the body to check general signs of health, including checking the penis for signs of disease, such as lumps or anything else that seems unusual. A history of the patient’s health habits and past illnesses and treatments will also be taken.
- Biopsy: The removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for signs of cancer. The tissue sample is removed during one of the following procedures:
- Fine-needle aspiration (FNA) biopsy: The removal of tissue or fluid using a thin needle.
- Incisional biopsy: The removal of part of a lump or a sample of tissue that doesn’t look normal.
- Excisional biopsy: The removal of an entire lump or area of tissue that doesn’t look normal.
After penile cancer has been diagnosed, tests are done to find out if cancer cells have spread within the penis or to other parts of the body.
The process used to find out if cancer has spread within the penis or to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment.
The following tests and procedures may be used in the staging process:
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerised tomography, or computerised axial tomography.
- MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. A substance called gadolinium is injected into a vein. The gadolinium collects around the cancer cells so they show up brighter in the picture. This procedure is also called nuclear magnetic resonance imaging (NMRI).
- Ultrasound exam: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram.
- Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
- Biopsy: The removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for signs of cancer. The tissue sample is removed during one of the following procedures:
- Sentinel lymph node biopsy: The removal of the sentinel lymph node during surgery. The sentinel lymph node is the first lymph node to receive lymphatic drainage from a tumour. It is the first lymph node the cancer is likely to spread to from the tumour. A radioactive substance and/or blue dye is injected near the tumour. The substance or dye flows through the lymph ducts to the lymph nodes. The first lymph node to receive the substance or dye is removed. A pathologist views the tissue under a microscope to look for cancer cells. If cancer cells are not found, it may not be necessary to remove more lymph nodes.
- Lymph node dissection: A procedure to remove one or more lymph nodes during surgery. A sample of tissue is checked under a microscope for signs of cancer. This procedure is also called a lymphadenectomy.
Penile Cancer Treatments
Key Points
- There are different types of treatment for patients with penile cancer.
- Four types of standard treatment are used:
- Surgery
- Radiation therapy
- Chemotherapy
- Biologic therapy
- New types of treatment are being tested in clinical trials.
- Radiosensitizers
- Sentinel lymph node biopsy followed by surgery
- Patients may want to think about taking part in a clinical trial.
- Patients can enter clinical trials before, during, or after starting their cancer treatment.
- Follow-up tests may be needed.
There are different types of treatment for patients with penile cancer.
Different types of treatments are available for patients with penile cancer. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Four types of standard treatment are used:
Surgery
Surgery is the most common treatment for all stages of penile cancer. A doctor may remove the cancer using one of the following operations:
- Mohs microsurgery: A procedure in which the tumour is cut from the skin in thin layers. During the surgery, the edges of the tumour and each layer of tumour removed are viewed through a microscope to check for cancer cells. Layers continue to be removed until no more cancer cells are seen. This type of surgery removes as little normal tissue as possible and is often used to remove cancer on the skin. It is also called Mohs surgery.
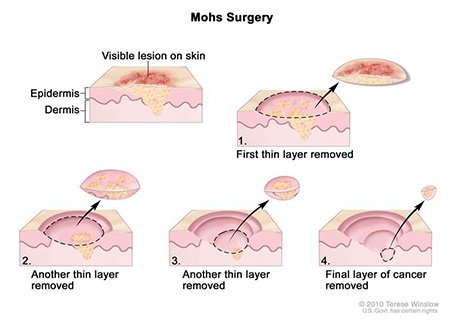
Mohs surgery. A surgical procedure to remove a visible lesion on the skin in several steps. First, a thin layer of cancerous tissue is removed. Then, a second thin layer of tissue is removed and viewed under a microscope to check for cancer cells. More layers are removed one at a time until the tissue viewed under a microscope shows no remaining cancer. This type of surgery is used to remove as little normal tissue as possible.
- Laser surgery: A surgical procedure that uses a laser beam (a narrow beam of intense light) as a knife to make bloodless cuts in tissue or to remove a surface lesion such as a tumour.
- Cryosurgery: A treatment that uses an instrument to freeze and destroy abnormal tissue. This type of treatment is also called cryotherapy.
- Circumcision: Surgery to remove part or all of the foreskin of the penis.
- Wide local excision: Surgery to remove only the cancer and some normal tissue around it.
- Amputation of the penis: Surgery to remove part or all of the penis. If part of the penis is removed, it is a partial penectomy. If all of the penis is removed, it is a total penectomy.
Lymph nodes in the groin may be taken out during surgery.
Even if the doctor removes all the cancer that can be seen at the time of the surgery, some patients may be given chemotherapy or radiation therapy after surgery to kill any cancer cells that are left. Treatment given after the surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy. External radiation therapy uses a machine outside the body to send radiation toward the cancer. Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer. The way the radiation therapy is given depends on the type and stage of the cancer being treated.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly onto the skin (topical chemotherapy) or into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). The way the chemotherapy is given depends on the type and stage of the cancer being treated.
Topical chemotherapy may be used to treat stage 0 penile cancer.
See Drugs Approved for Penile Cancer for more information.
Biologic therapy
Biologic therapy is a treatment that uses the patient’s immune system to fight cancer. Substances made by the body or made in a laboratory are used to boost, direct, or restore the body’s natural defences against cancer. This type of cancer treatment is also called biotherapy or immunotherapy. Topical biologic therapy with imiquimod may be used to treat stage 0 penile cancer.
New types of treatment are being tested in clinical trials.
This summary section describes treatments that are being studied in clinical trials. It may not mention every new treatment being studied. Information about clinical trials is available from the NCI website.
Radiosensitizers
Radiosensitizers are drugs that make tumour cells more sensitive to radiation therapy. Combining radiation therapy with radiosensitizers helps kill more tumour cells.
Sentinel lymph node biopsy followed by surgery
Sentinel lymph node biopsy is the removal of the sentinel lymph node during surgery. The sentinel lymph node is the first lymph node to receive lymphatic drainage from a tumour. It is the first lymph node the cancer is likely to spread to from the tumour. A radioactive substance and/or blue dye is injected near the tumour. The substance or dye flows through the lymph ducts to the lymph nodes. The first lymph node to receive the substance or dye is removed. A pathologist views the tissue under a microscope to look for cancer cells. If cancer cells are not found, it may not be necessary to remove more lymph nodes. After the sentinel lymph node biopsy, the surgeon removes the cancer.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today’s standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. See the treatment options section that follows for links to current treatment clinical trials. These have been retrieved from NCI’s listing of clinical trials.
Follow-up tests may be needed.
Some of the tests that were done to diagnose the cancer or to find out the stage of the cancer may be repeated. Some tests will be repeated in order to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back). These tests are sometimes called follow-up tests or check-ups.
Treatment Options by Stage
Stage 0 (Carcinoma in Situ)
Treatment of stage 0 may be one of the following:
- Mohs microsurgery.
- Topical chemotherapy.
- Topical biologic therapy with imiquimod.
- Laser surgery.
- Cryosurgery.
Stage I Penile Cancer
If the cancer is only in the foreskin, wide local excision and circumcision may be the only treatment needed.
Treatment of stage I penile cancer may include the following:
- Surgery (partial or total penectomy with or without removal of lymph nodes in the groin).
- External or internal radiation therapy.
- Mohs microsurgery.
- A clinical trial of laser therapy.
Stage II Penile Cancer
Treatment of stage II penile cancer may include the following:
- Surgery (partial or total penectomy, with or without removal of lymph nodes in the groin).
- External or internal radiation therapy followed by surgery.
- A clinical trial of sentinel lymph node biopsy followed by surgery.
- A clinical trial of laser surgery.
Stage III Penile Cancer
Treatment of stage III penile cancer may include the following:
- Surgery (penectomy and removal of lymph nodes in the groin) with or without radiation therapy.
- Radiation therapy.
- A clinical trial of sentinel lymph node biopsy followed by surgery.
- A clinical trial of radiosensitizers.
- A clinical trial of chemotherapy before or after surgery.
- A clinical trial of new drugs, biologic therapy, or new kinds of surgery.
Stage IV Penile Cancer
Treatment of stage IV penile cancer is usually palliative (to relieve symptoms and improve the quality of life). Treatment may include the following:
- Surgery (wide local excision and removal of lymph nodes in the groin).
- Radiation therapy.
- A clinical trial of chemotherapy before or after surgery.
- A clinical trial of new drugs, biologic therapy, or new kinds of surgery.
Treatment Options for Recurrent Penile Cancer
Treatment of recurrent penile cancer may include the following:
- Surgery (penectomy).
- Radiation therapy.
- A clinical trial of biologic therapy.
- A clinical trial of chemotherapy.